You're gonna want to know about this.


In conjunction with attitudinal changes, new technology has opened up alternatives. For breast cancer patients, surgeons can now offer cutting-edge innovations.
One of the top things a doctor can do for a patient is to empower them to be part of the decision-making process by giving them a full range of options around their treatment. The days of paternalistic practitioners are in decline. In conjunction with attitudinal changes, new technology has opened up alternatives. For breast cancer patients, surgeons can now offer cutting-edge innovations.
The radioactive breast seed, for example, enables a surgeon to locate abnormal tissue too small to be felt by human touch (non-palpable). It leads the doctor to the location of cancerous tissue, yielding the target area for surgical action with precision.
For those who have been diagnosed with early stage breast cancer and are considering a lumpectomy as a breast-conserving surgery, there is the MarginProbe. It “enables real-time detection of cancer” in the operating room, during the lumpectomy process. Dune Medical Devices, the creating company, calls it an “intraoperative assessment tool.” Previously, an almost a seven-day wait time had to be endured before lumpectomy patients received results from a pathologist. Then, if the margins from the excised tissue were not clean and free from cancer, a follow-up surgery was necessary.
The MarginProbe system is FDA approved and has gone through two iterations. Revisions were based on feedback from surgeon use, along with the integration of tweaked design elements.
The system uses radio frequency signals to measure the difference between normal and malignant breast tissue (I visualized it as being similar to a Geiger counter).
I reached out for more background to Gil Rosen, Chief Commercial Officer at Dune Medical Devices. Via email, he sent me additional information in response to questions, as well as several studies.
Currently, over 90 MarginProbes are in use in the United States. The cost of the tool is $1,200 per surgery. “Many of our customers [hospitals] are routinely reimbursed,” Rosen wrote.
Since the tool was introduced, it has been used 4,000 times. Rosen related that 400 procedures are performed each month, and that the growth rate is “in the double digits quarterly.”
In the 2013 German “post-market study” I looked at, the authors concluded that the MarginProbe had lowered the re-excision rate for ductal carcinoma in situ (DCIS) and invasive cancer by 50%. This is a breakthrough statistic.
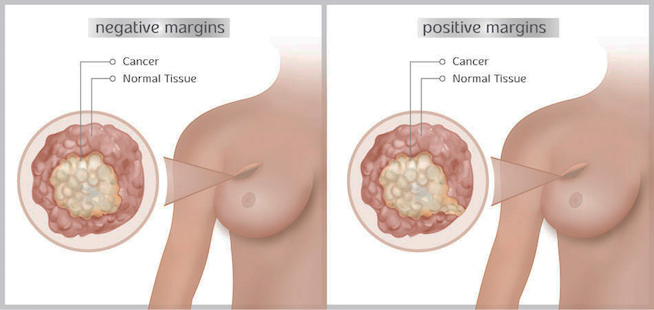
Taking into consideration that today’s patients are proactive in seeking information, MarginProbe has put together an extensive website that provides information including data and a drill down explanation of how the MarginProbe works. It has mapped where doctors using it can be found (There were numerous contacts in my area of New York City). What was most beneficial was a clear definition of the terminology, “negative margins.” The site clarifies: “The objective [of a lumpectomy] is a clean, negative margin, with all six surfaces of an excised tumor cancer-free.” When I saw the medical illustration, the visualization made everything simple and comprehensible.
Patients who have cancer in both breasts, or who have had prior radiation or surgery in the affected breast, are not candidates for this technology.
One of the surgeons using the MarginProbe is Dr. Erica Giblin. She works at the St. Vincent Carmel Women’s Center in Indiana and specializes in breast conservation surgery. When I interviewed her by telephone, she emphasized, “It is very important to make sure you get all the cancer out. This tool helps us a lot in this regard.”
Discussing the differences in how women choose to approach their diagnosis, Giblin noted that many women see their breasts as an integral part of their identity. These patients want to avoid a maximum surgery. “Patients want to have one procedure and be done,” Giblin said. “I looked through the data on the tool and believed it would have utility.” She added, “My experience has been good.”
Within the time frame Giblin has been using the MarginProbe, she has found that the lower incidence of re-excision has been promising. She describes to her patients how the probe works, to “make sure the margins are clean and no cancer is left behind.” Without this methodology, the odds are 25%that a surgeon will have to bring the patient back into the operating room. Giblin explained that with the probe, the odds for that necessity go down to 12.5%. For Giblin, the goal is to accomplish what is necessary in ”only one go around.”
Her bottom line was succinct: “We’re trying to get as accurate as we can.”